


What is the White House doing about overdose deaths?
President Biden calls for harm reduction, but also requests the largest ever funding increase for Customs and Border Protection and the DEA. Plus, new harm reduction polling from Data for Progress.

President Joe Biden’s White House just released the 2022 National Drug Control Strategy aimed at addressing the skyrocketing rate of overdose deaths in America. A Fact Sheet summarizing the strategy zeroes in on “two critical drivers of the epidemic.”
The two main drivers identified in the new strategy are “untreated addiction” and “drug trafficking.” I want to walk through the national strategy to suss out what the plan actually entails and whether or not it will meaningfully address this dire problem that has eluded President Biden’s predecessors. Since 1999, more than one million people have died from drug overdoses. When the hell is this going to end? What’s it going to take to finally make a dent in this emergency?
290 people are dying everyday in America from largely preventable deaths. The same old drug policy is not gonna work.
The 2022 national strategy identifies “drug trafficking” as a major driver of overdose deaths and proposes the largest ever increase in funding for Customs and Border Protection (CBP) and the Drug Enforcement Administration (DEA).
The Strategy builds on the President’s FY 23 budget request for a $300 million increase to support the work of Customs and Border Protection (CBP)–one of the largest ever increases for CBP–and for a $300 million increase for the Drug Enforcement Administration.
Policing the border doesn’t sound like a particularly new or effective strategy. In fact, America has claimed to be doing exactly this all the while drugs have become cheaper, more potent, and more accessible—the exact opposite outcomes one would expect from a successful supply-side drug strategy. The big idea animating America’s supply-side drug policy for decades is that huge drug seizures will result in illegal drugs becoming scarce and more expensive. The drugs on the street will then get diluted and crappy, driving down the potency while upping the cost and people addicted will get fed up, stop wasting their time and money on pursuing garbage drugs, and enter treatment.
Something sort of like this happened a while ago in Australia. In 2001, there was a sudden heroin drought and the street supply nearly disappeared as a result of huge seizures made by law enforcement. The heroin supply became expensive and the quality went down and more people started treatments like methadone. Though other people just switched drugs and the supply shock didn’t make a huge difference. While Australia is an interesting case, it doesn’t really map on to the realities of America today. Australia is a remote island that doesn’t share a border with Mexico, for one.
As far as I’m aware, the DEA and other law enforcement groups in the US have never come close to eliminating the illicit drug supply. In my ten years studying American drug markets, I’ve never heard of a drought on the level of Australia. Whether you’re in Baltimore, Philly, Chicago, LA, Phoenix, New York etc. there seems to be a never ending supply of drugs.
And that’s been the status quo while the DEA’s budget has ballooned to over $3.1 billion. Now, President Biden wants to give them more money for a job they are demonstrably bad at doing. The DEA couldn’t even keep close watch on American pharmaceutical companies selling substances ostensibly “controlled” by the DEA. How on earth is this agency going to make a dent in drug trafficking organizations? When I royally fuck up I tend to not get a huge raise from the president of the United States.
What has the DEA been doing with all this money? I’m glad you asked:
Having wild sex parties in Colombia (sounds neat, but not very helpful)
Paying confidential informants exorbitant fees with little oversight
Secretly intercepting millions of texts and phone calls on dubious legal grounds
Look, the contaminated drug supply is actually a serious problem and it’s causing tons of needless and tragic deaths. Drug trafficking is no doubt an obvious part of this mess. But it’s a mystery to me how giving more money to these agencies is going to somehow a) eliminate the contaminated market and b) reduce overdose deaths.
Changing gears, here. That was the supply side of the equation, which America tends to prioritize and pour money into. Let’s look at the other side of the equation.
President Biden’s new drug strategy identifies “untreated addiction” as a major driver of the overdose crisis. The section begins with data about the population of people who have a substance use disorder and the lack of treatment they’re receiving. The strategy cites government reports showing 41.1 million people needed treatment for an SUD, but only 2.7 million (6.5-percent) of them received treatment. That’s a huge gap! “One reason for this gap is that people with addiction and those who care for them face too many barriers to treatment,” the report states. That’s true, but I think it’s much more complicated than that.
First, it’s important to recognize that not everyone who uses substances meets the clinical criteria for a substance use disorder (SUD) diagnosis. Moreover, not everyone who meets criteria for an SUD actually needs treatment. So that 41.1 million people sounds like a huge number, but it’s probably over-counting the number of people need treatment. It’s simply not the case that all these people overdosing have a SUD. In fact, it’s probably more likely that people who are overdosing do not have a high tolerance for these potent synthetic opioids and may not even be addicted to them.
For those who are addicted, there’s some serious problems with addiction treatment in America. Dr. Rahul Gupta, who leads President Biden’s drug policy, recently said that America basically doesn’t have any real addiction treatment infrastructure to speak of. What we have is a haphazard patchwork of state-run and private facilities that don’t adhere to the same standards; some treatment facilities seem to have zero standards at all.
Everyone is kinda doing their own thing, so it’s pretty impossible to really know what “treatment” is out there, and it’s even harder to separate quality medical treatment ran by professionals from shoddy quacks who open up a treatment facility in a Florida strip mall and bill insurance companies thousands of dollars for unnecessary drug tests and treatments that don’t really work. Finger-painting and doing yoga on the beach sounds relaxing, but it is not treating your addiction.
America’s treatment patchwork also continues to prioritize abstinence over all other outcomes, and this is another major problem, especially in the world we live in with highly potent opioids out there. Dr. Nora Volkow, who leads the National Institute on Drug Abuse, summed it up well:
“The magnitude of this crisis demands out-of-the-box thinking and willingness to jettison old, unhelpful, and unsupported assumptions about what treatment and recovery need to look like. Among them is the traditional view that abstinence is the sole aim and only valid outcome of addiction treatment.
Temporary returns to use after periods of abstinence are part of many recovery journeys, and it shouldn’t be ruled out that some substance use or ongoing use of other substances even during treatment and recovery might be a way forward for some subset of individuals.” - Nora Volkow
When the leader of the world’s largest addiction research agency is taking time out of her busy day to call out the organizing principle and North Star of America’s treatment industry as outdated and flawed, you know there’s a problem.
And since we’re talking mostly about overdose deaths caused by potent synthetic opioids like illicit fentanyl—though it’s important emphasize the role of polysubstance overdoses, aka drug mixing—America’s patchwork of treatment is uniquely ill equipped to treat opioid use disorder. Only 11 percent of people with opioid use disorders receive one of only three FDA-approved medications. Yup, there’s only three medications people have to choose from and they’re barely accessible. Furthermore, only two of those medications—methadone and buprenorphine—are associated with reducing the risk of fatal overdose. Until America’s treatment facilities and the federal government remove barriers that get in the way of these medications, there’s no end in sight for this crisis. If a $5 bag of a highly potent synthetic opioids is easier to get than methadone or buprenorphine, frankly, we’re screwed.
There may actually be some good news coming down on this front. Biden’s drug policy is genuinely trying to make medications more accessible through low-barrier programs. In other countries, methadone is treated mostly like any other drug. People go to a pharmacy, pick it up, and go about their day. But not in America. Right now, during this emergency, people can only obtain methadone through a Kafkaesque system of national clinics. These clinics can make life a living hell for people.
As RAND’s Bryce Pardo points out below, a review of methadone regulations is currently underway and that might just finally lead to much easier access to a medication that can drastically reduce the risk of fatal overdose. I don’t know what they’re waiting for! Liberating methadone from these burdensome regulations rooted in stigma should’ve happened long ago.


OK. Back to “untreated addiction.”
If so many people who need treatment aren’t getting it, is it maybe because they don’t want the treatment that’s being offered? What about the people who’ve tried the same treatment over and over again and it hasn’t worked? I’ve talked to countless people who are in this boat. They’re trapped in the illicit drug market, injecting cheap synthetic drugs that are now laced with tranquilizers or benzodiazepines, and they see no way out.
The conventional buprenorphine induction is made very complicated by illicit fentanyl. People go through agonizing withdrawals when they try to start buprenorphine because these illicit fentanyls stay in their bodies for so long, triggering what’s called precipitated withdrawal, which I can only describe to you as a syndrome of pure hell, the longest waking nightmare you’ll ever experience.
People are scarred by the experience and they don’t want try it again. People using drugs aren’t dumb! Why would they sign up for a program that is probably going to make them feel miserable, where they’re sick from withdrawal and aren’t getting the relief they need, and the one thing that will make them feel better (temporarily at least) is just a stroll down the street?
As I’ve said, the dominant treatment paradigm in America remains to be abstinence and Twelve-Step based, which usually means a 28-day residential program like you see on TV, where people spend upwards of $30,000+ per month petting horses on a Malibu ranch, come home, and immediately relapse. If America wants to reduce the size of the “untreated” population, then there needs to be a drastic change to what passes for treatment.
For more on that, check out Jeff Deeney’s thread, in which he correctly labels America’s treatment as “trash.”

I know, I know. You’re sick of hearing me saying this by now but the drug supply is contaminated. This situation is unprecedented and it demands new ideas, new strategies, and yes, things that for the average American might be hard to swallow.
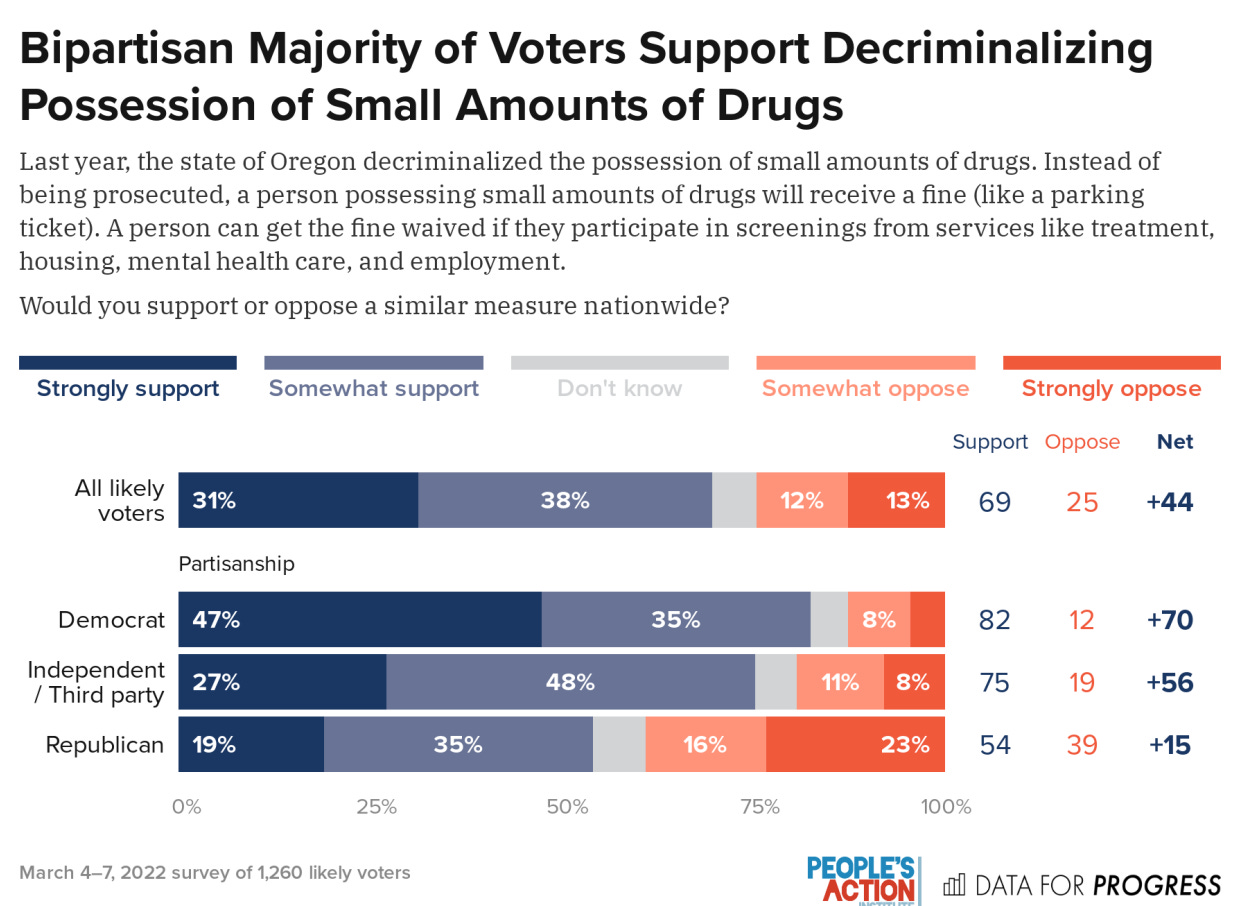
But there is some new polling about harm reduction by Data for Progress and People’s Action that finds people are more open and receptive to these ideas than you might think. One of the big findings from this new polling that jumped out to me is just how widespread substance use and overdose is in America. Nearly half of voters have some personal experience with this issue.

On harm reduction, voters also widely support it. Among voters polled, 64 percent support opening overdose prevention centers.

There is also majority and bipartisan support for new drug policy overall. Voters support policies like drug decriminalization. There is also huge support for naloxone distribution and increased access to medications that save lives. With 290 people per day dying, there is both massive need and public support to do way more about this issue.
President Biden’s drug policy strategy does identify the need for much more harm reduction, especially wider distribution of naloxone along with robust local syringe service programs. These are popular among voters. But what I don’t get is why $600 million more dollars is going toward the DEA and border patrol, agencies that already have bloated budgets and haven’t accomplished much of note with it.
The Biden administration would get much more bang for their buck by pouring that $600 million into building a national harm reduction infrastructure. It makes much more sense to spend money on things that actually help people. Like building up local syringe programs in hard-hit communities, where people can get naloxone and other services they need, where people feel seen and understood and comfortable. With their massive budget and fancy tools, how many overdoses deaths has the DEA really prevented?
Local harm reduction programs that actually care about people who use drugs and make them feel welcome could be the first door people walk through on their way toward a better, fuller, healthier life.
In the 152 pages of Biden’s drug strategy, there was no mention of supervised consumption sites or overdose prevention centers, and no mention of prescription heroin or injectable opioid agonist therapy. In a crisis as serious as the one we’re in, shouldn’t we be trying everything we can to save lives? Harm reduction strategies and ideas like prescription heroin have solid evidence supporting them, but evidence is not enough to make them magically appear. America’s drug policy is stuck, and that means we’re stuck living in this tragedy.